What's the difference between a fairy tale and a sea-story? A fairy tale begins, "Once upon a time..." A sea story begins, "This is no shit!"
I try to be careful to change names, but to the best of my recollection the events and locations are substantially correct. Of course I can only describe events from my perspective, so there's that. Readers who were present will doubtless have different recollections of any particular event. This is what it was like to serve in my tiny slice of the U.S. Navy between the late 1970's and early 1990's. It really was an adventure.
Remember,
This is no shit!
It was one of those lovely, quiet times on the ship, zero dark thirty and only a few hundred souls awake. USS Boat was swinging on the hook at Haifa, Israel, counting down the last few hours of a delightful port visit. I'd worked nights on the Beach Guard detachment during most of the stay and had only just returned to the ship. I was in sick bay down on the second deck, and I'd just finished inventorying, replacing and stowing the Beach Guard first aid gear.
Sick bay -- also known as H-Division or Medical -- was located right in the guts of the carrier. The hangar bay was the first, or "main" deck, and sick bay was below the hangar bay on the second deck, right on the centerline of the ship. Forward of sick bay was the forward galley and mess decks, and aft was -- perhaps unsurprisingly -- the aft galley and mess decks. Forward and aft of the mess decks there were scores of little shops and offices and vast berthing areas where hundreds of men lived in three-high "coffin" racks. A pair of fore-and-aft passageways ran the length of the second deck on each side -- port and starboard -- of sick bay.
As an aside, all of the "floors" from the hangar bay/main deck on down were called decks and numbered first, second, third, etc. Those above the main deck were called levels and were numbered oh-one, oh-two, oh-three, etc. The flight deck was the oh-four level.
There aren't a lot of quiet moments on a warship on deployment. The quiet wouldn't last; as soon as the sun rose over the Holy Land we'd be leaving port. In a couple of hours they'd call away the special sea and anchor detail, raise the hook, and the carrier would depart Haifa and get on with all the navy stuff. For the moment, however, all was quiet. Most of the crew were snug in their racks, catching a few final hours of peaceful (in some cases ethanol induced) sleep before the onset of a busy underway period.
The two junior guys of the medical department watch section were playing cards in the medical records office.
The section leader was in the pharmacy (he was the pharmacy tech) writing a letter.
The rest of the watch section were crapped out on cots back aft in the medical ward.
I finished stowing my gear and wandered into the treatment room to study.
I'd need to man the flight deck battle dressing station when they called away sea and anchor in a couple of hours, but for the moment I was comfortable in sick bay reading up on Mediterranean parasitology. Do you have any idea what mosquitoes put into you when they bite?
I heard the portside sickbay door open and close, followed by low voices. Then a sudden shout. "Help!"
Oh shit.
##########
It was cruise number four for me, and fairly early in the deployment. We were back in the Mediterranean, and it was interesting times indeed.
U.S. aircraft carriers had been a constant presence in the Mediterranean since the end of WWII, protecting Europe's soft underbelly from Soviet aggression. That was our main brief, to be prepared to conduct war at sea against the Soviets, and, if it came down to it, to execute our part of the SIOP.
A lot of people have been katie couric'ed into believing that there was never really any cold war, just a bunch of hateful American imperialists swinging phallic symbols all over the place and oppressing the po' folk of the world. That the peaceful soviet peoples were simply building tractors and trying to bear up under the mean and racist policies of the evil George W. Hitler who was, at the time, working through his proxy-puppet Ronald Reagan. The Russians, so couric tells us, were far too poor to have a real military, and certainly didn't have a blue water navy.
Those of us who were there know different. Though they had no aircraft carriers, the Soviets usually had as many, if not more, warships operating in the Med as the U.S. Navy. Cruisers and destroyers in the main...
...along with a handful of submarines and a few AGI's. So yeah, mostly a bunch of dugout canoes.
The AGI's were intelligence gathering platforms, often called "trawlers" by couric and her ilk, as if they were nothing more than peaceful commercial fishing vessels. We'll take a closer look at them in a future post.
The Soviets may have had no carriers (YAK-38/VTOL cruisers don't count, sorry), but that doesn't mean they lacked air power. There were significant naval aviation assets nearby in the Black Sea area, and the Soviets frequently operated aircraft out of Syria, Egypt, and Libya.
In reality, any U.S. - Soviet punching match in the Med would be a very big, very serious fight. And as if that wasn't enough...
There was Khaddafi in Libya. In addition to hosting a lot of Soviet airpower and allowing the Soviet navy port and maintenance facilities, he was exporting terror and constantly probing our Sixth Fleet defenses. That was the southern Med. In the east...
Lebanon. Just the name makes my palms sweat. There'd been a three-way civil war going on in Lebanon since 1958. Nothing is as it seems in that part of the world, though, so it was actually more like a 14- or 15-way civil war. Sunni and Shia, of course, Maronite Christians and Druze. Those were the locals. Then there were the illegal aliens; Palestinians and various exiled Islamic groups from Syria, Jordan and Iran. And let's not forget the commuters; military forces from Syria, Jordan, Egypt and Israel. There were contract mercenaries from Europe -- from both sides of the iron curtain -- and even mercenaries from America. And of course there were the big boys; the U.S. and France (Lebanon is a former French colony), each of which fielded both regular and special forces at various times. And the U.N. With the exception of the Iran-Iraq battlefields, Lebanon was the deadliest place on earth from about 1975-1995.
At the time this tale begins, various factions of an amorphous militant group called Islamic Jihad were keeping dozens of western hostages in and around Beirut. More than two dozen were American. There would also be a hijacking a few short weeks later, with the hostage-packed TWA 727 spending some time on the ramp at Beirut International. All of this Lebanese turmoil would mean that we'd spend most of our deployment in the eastern Med, and that I'd once again have the opportunity to visit the former "Pearl of the Mediterranean."
All of that was in the future and would come to overshadow the first weeks of the deployment, which had already been more eventful than usual.
##########
The morning we pulled into Haifa, I'd mustered with the rest of the Beach Guard detachment in hangar bay three. We'd be the first of the crew ashore and would set up a check point and control area at fleet landing. We'd be the ship's official presence ashore at the point where sailors on liberty would debark and embark from the liberty boats ferrying them ashore. The ship was far too large and drew too much water to come alongside the piers in the harbor.
Beach Guard was great duty. There were watches to stand, of course, and you had to be available for recall so no extended tours away from the city, but it also featured free lodgings in a nice hotel, generous per diem, and relief from regular one-in-three watch standing on the boat.
As we mustered on the hangar deck the ship's XO appeared and the Beach Guard OIC called us to attention.
"Okay fellas," said the XO, "when you get ashore there's going to be a lot of press with a lot of questions. Just tell 'em you don't know anything and refer 'em to the PAO. That should be easy, because you don't know anything, even if you've heard something or think you know something. Let me be very clear. You do not want me to read your name in the papers."
Well. This wan't my first rodeo, but the XO's little spiel was a first for me. I wondered what it was all about.
As promised, there was a lot of press ashore. The officers and Chiefs did a fine job of running interference for us, and I was a past master at looking like I was way to busy doing something really important to be bothered, so I was never in danger of being quoted.
Over the next few days we read the papers and listened to the scuttlebutt and gained some understanding of what had happened. Few, if any of us, had ever heard of or even seen Michael Walker.
Another thing we didn't know anything about was the fact that NIS (naval investigative service) had, on the first day of the port visit, cracked a drug ring on the ship. That was really a surprise to me, and actually made a bigger impression on me than the spy thing.
I was probably a real naif at the time (probably?!?) but when the CNO came out with "Not on MY watch, not on MY ship, not in MY Navy" I bought in completely. I knew there were dopers around, most of whom stuck out like a diseased tool. They were slovenly noloads as far as I could tell, and their behavior put me and my shipmates in mortal peril. I agreed wholly with the fleet solution to drug use. Send them firetruckers back to civilianland!
IIRC, Operation Golden-flow hit high gear back in '81, following the EA-6B crash on Nimitz. It slashed through the doper community like a scythe through rotting grain, and my fleet and my navy got better and better and better. By 1985 you just didn't see dopers anymore. Well, I didn't see dopers anymore. I'd pretty much forgotten all about them.
But they were still there...
##########
Now where was I? Oh yeah.
Oh shit!
I came left out of the treatment room and left again. This put me in the port-starboard transverse passageway that ran right through sickbay. The two duty corpsmen were huddled around a dungaree-clad sailor who was sitting on the deck with his back to the bulkhead.
Behind him a smear of red ran vertically down from about chest height. The sailor was a first class petty officer, and one I'd seen around from time to time. He was shaking his head and moaning softly.
The two junior corpsmen were starting to panic. Neither worked in patient care; one was a medical supply clerk and the other worked in medical records.
The supply corpsman was standing back, looking at the blood on the wall with big eyes. I shall call him, for the purposes of this post, Danny Dumbf... er, Danny. He was a sawed-off, little banty rooster of a fellow who did a lot of weight lifting and had dreams of not getting sand kicked in his face ever again. The records corpsman was on his knees next to the slumped E-6, trying valiantly to blow a whistle.
Blow a whistle?
Yes, blow a whistle. At some point in the past, apparently, a lone corpsman had been presented with a middle-of-the-night emergency and had gone looking for help, leaving a sick or injured sailor to his own devices. Thereafter a shiny whistle was installed in the medical records office (first stop for anyone visiting sick bay) and everyone was instructed that should they find themselves in a similar situation, they should stay with the patient and blow the whistle to summon help.
But the poor records guy, who I shall call Bobby, couldn't work the whistle in his panic.
##########
Panic is one of those funny things. You simply can't be prepared for your first real emergency. You can know your stuff cold and have talked it through and thought it through and done drills out the wazoo, but the real thing is different.
My first real emergency was a simple one. I was still in Corps School (Basic Hospital Corps School) and doing a rotation on the wards at Balboa Naval Hospital. I was "assisting" Dr. Somthinerother who, if I was reading his shoulder boards correctly, was a freaking 0-5 Commander fer crying out loud! I was only a couple of weeks out of boot camp and the most senior officer I'd been this close to thus far in my career was an 0-3 Lieutenant. I'd only ever spoken to one officer, an Ensign, and the conversation had gone something like this:
"Are you getting enough chow, Recruit?"
"YESSIR!"
And here I was suddenly and unexpectedly rubbing shoulders with a Commander or Admiral or some shit!
Dr. Somthinerother had just given a patient a shot of demerol and the patient was trying very hard to stop breathing.
"Get me some narcan," snapped the Commander.
I panicked. I knew instantly that this was an emergency. But I had no idea what narcan was; whether it was medicine or medical gear or sandwich spread. I'd clearly been given an order, and it was clearly a damned important order, but I didn't know what it meant and I didn't know what to do. I stood there, rooted to the ground, mind spinning uselessly, and doing absolutely firetruck-all.
The Commander looked at me, rolled his eyes, and bellowed.
"NURSE, NARCAN!"
Well, Nurse JayGee knew what narcan was and came dashing in to save the day. For the patient, anyway. As for me, I had visions of suddenly becoming a non-designated Seaman Recruit and spending the next four years chipping paint.
Later Nurse JayGee gave me a stern but kindly lecture about emergencies and panic. Which I took to heart.
##########
"Arright," I said, "let's get him in the treatment room." I bent down and grabbed the injured fellow's arm.
I'd already done a quick and dirty field assessment. He was conscious and alert, probably more scared than in genuine pain. He was breathing spontaneously and well, and while he was obviously bleeding, he wasn't bleeding a lot, at least externally. We really needed to get him into the treatment room and onto an exam table, the sooner the better. There was no need to go through all the stretcher rigmarole to move him 30 feet, and the way he moved would provide more detail for my initial assessment.
Bobby and I got the fellow up and moved into the treatment room. I sent Danny to call the duty doc, CDR Portly. I helped the injured guy out of his shirt and had Bobby start taking vital signs. Then I got my first look at the wound.
It was a half-inch slit, about 5-6 inches down from the top of the back, 3 inches to the right of the spine, just slightly above and to the left of the lower point of the shoulder blade. The wound had already stopped bleeding. With every breath the fellow took, though, a couple of bloody bubbles formed in the wound.
Ruh-roh. Sucking chest. Not a bad one -- at least not yet -- but a sucking chest wound nonetheless. Now how in the hell...
"What happened?"
"Motherfucker stab me."
A quick game of 20 questions revealed that the guy had been getting up for watch from his rack in one of the 99-man berthing areas. For some reason all the lights were out, and as he stumbled around someone had knifed him in the back, then fled.
Well shit! A firetrucking stabbing? Here, on the boat? WTF?
"Danny, call the MAA's. And where the hell is CDR Portly? What did he say when you called him?"
As it turned out, Danny hadn't called the duty doc at all. The whining excuses began to flow.
"Never mind," I said, "Go get HM1 Pharma, ask him to come to the treatment room. Do you understand that? Where are you going to bring HM1 Pharma?"
"Yes. Treatment room." Pouting and sullen.
I picked up the phone. I called CDR Portly first.
"Sorry to bother you, Doc, but we got a guy down here who's been stabbed in the back."
"Whaa..., what?"
"Got a guy with a sucking chest, he's been stabbed in the back."
"In the back of what?"
"In the back of his front! Oh, hell, never mind."
I hung up and called LCDR Sharp, the Ship's Surgeon. He was the one we really needed anyway, and Portly would likely just slow things down and firetruck things up.
"Be right there," said the surgeon.
The section leader rolled in with Danny in trail. I briefed him, then picked up the phone to call the MAA's.
"In the back of what?"
Firetruck me, I thought, this is gonna be one of those days.
##########
Sucking chest wound. Here's how it works.
Your lungs are, obviously, in your chest cavity. The left one has two lobes, the right one has three. For our purposes we'll just consider them to be two lungs. They're connected to the outside via the windpipe, which leads to the mouth and nose. Inside the lungs the windpipe branches and branches and branches, becoming the bronchus, the bronchial tubes, and finally the alevoli, teeny-tiny sacs where oxygen and carbon dioxide are exchanged. Far from being hollow balloons, the lungs are actually fairly solid organs, filled with passageways, blood vessels, and specialized tissues. They're obviously less solid than other organs, and just as obviously hold a lot of air (even when you try to blow it all out), but they're much more than simple air-filled bags.
Now whether you're breathing in or out, whether you've taken a deep breath or have exhaled every bit of air you can, your lungs remain fully expanded in the chest cavity, filling it completely. The thing that allows you to breathe in and out, to take air into the lungs and exhale air out of the lungs, is a simple change in the geometry of the inside of the chest. When you breathe in, the diaphragm pulls down, expanding the volume of the chest cavity. When the volume expands, the pressure inside the chest falls, and air flows in. When you exhale, the reverse happens.
As noted before, the lungs are always completely expanded in the chest cavity, taking up the entire space allotted to them. This is because there is always a slightly negative pressure in the pleural space, which lies between the outside of the lung and the inside of the chest wall. The pleura is the specialized tissue which lines the inside of the chest cavity and the outside of the lungs. It's quite tough and air tight and continually secretes a lubricating fluid which allows the lung and chest wall to move against each other with very little friction. The slight negative pressure in the pleural space between the lung and the chest wall keeps the lungs ever expanded.
So the lungs are always expanded, except when that negative pressure in the pleural space is lost. That can happen in two ways. The lung can leak air into the pleural space, or some kind of trauma (a knife wound, for instance) can allow air from the outside to leak into the pleural space. In some instances (like a knife wound), the trauma might do both, letting in outside air as well as inside air from a damaged lung.
When air leaks into the pleural space and the negative pressure is lost the lung can no longer remain completely expanded in the chest and it begins to collapse. As long as air can move freely in and out of the pleural space, the lung can still function, after a fashion, but at greatly reduced efficiency. However, if air builds up in the pleural space the increased pressure will eventually crush the lung to uselessness, and if it continues unchecked can actually squeeze the heart, great vessels of the chest, and the other lung into uselessness too. Which is bad.
Trauma can also allow blood to fill the pleural space, and since liquids don't compress, this condition can be much more severe and can happen very rapidly.
If there's air in the pleural space, the condition is called a pneumothorax. If it's blood, it's called a hemothorax. If both air and blood, it's a pneumo-hemothorax. If pressure builds up it's a tension pneumo, hemo, or pneumo-hemothorax. In any combination the lay term is collapsed lung, and in any combination it's a very serious condition and generally treated as a medical emergency.
##########
On exam the guy was an otherwise healthy male, about 30 years old. His vital signs were normal with the exception of a slightly fast pulse, about 100 beats per minute. He was alert and oriented and answering questions. He acted a little more depressed than excited. He kept his face mostly pointed toward the deck and didn't want to make eye contact.
Other then the wound in his back he had no injuries. When I listened to his chest I could hear good breath sounds on the left but no breath sounds on the right. His heart sounded good. His trachea was midline, which was good. If pressure was building in his chest the trachea would eventually begin to shift shift. It looked very much like he had a relatively uncomplicated traumatic pneumothorax. He'd been very lucky.
The pneumothorax was still going to have to be fixed, though, So I went ahead and started an IV and drew labs. I sent Bobby off to wake up the lab tech and the x-ray tech.
LCDR Sharp rolled in, examined the injured sailor, and reached the same conclusions I had. Which is not to say that my conclusions were in anyway brilliant. It was pretty darned obvious.
Dr. Sharp wanted to take the guy to OR to fix the problem, so he sent Danny off to round up some OR techs and picked up the phone to call LT Jones, the ship's nurse anesthetist.
"Do we have x-rays yet?"
About that time Bobby rolled back in with the lab tech and reported that the x-ray tech was still too drunk to function.
Which wasn't any real problem, because I could shoot and develop the chest films. Which I did (If you'd like to see a slideshow of chest radiography, this is a pretty good one). When I brought the x-rays out of the darkroom, however, the treatment room was crowded with MAA's and a number of rather senior officers. It was pandemoneous!
Listening to the conversations and to the questions the MAA's were asking the injured sailor, it didn't take long to figure out what was going on. Our patient was one of the guys snapped up in the drug investigation and had been "cooperating with the authorities." Apparently this was not appreciated by some segment of the ship's drug culture. Which had heretofore been completely invisible to me.
To the me of that place and that time, the whole thing was shocking and confusing. I suppose that at some intellectual level I realized that in any small town of 6,000 souls there would be some lawbreakers. But for god's sake, murderers? There were people on my boat who would actually kill a shipmate, or at least give it the old college try? Good lord! The situation was an eye opener and, in some ways, one of the more painful lessons of growing up.
It was rather amusing to watch and listen to the ship's crack team of investigators though. MAA's, or Master at Arms, are the navy's police force. I think things have changed a lot since 1985, and I can't speak to today's practices, but back then most of the ship's MAA force were temporarily assigned to the duty and received a very basic level of training, followed by OJT. Only very senior MAA's received formal training, and my guess is that such training was weighted more toward the administrative aspects of law enforcement rather than the investigative.
The upshot, IMO, was that in a "big" and "exciting" situation such as attempted murder, our MAA force turned into a bunch of kids playing cops and robbers. That's not to say they weren't competent or that they weren't doing a fine and necessary job, but I'm here to tell ya that the treatment room was awash with all the cop characters from ADAM-12 and Dragnet that morning.
##########
We still had an injured sailor to deal with, so the surgeon invited all the giddy pseudo cop thespians to take their show on the road. The Chief MAA couldn't keep himself from playing a couple of rounds of "who's the big dog," which he lost. As a concession, he was allowed to leave two of his men behind to provide "security" and to record the patient's "dying declaration." If it came to that. Which it wouldn't, but the Chief was a big fan of ADAM-12.
"Well," said Dr. Sharp, "If officers Malloy and Reed are gonna be here, we can't use the OR. Not enough room. So we'll do it here in the treatment room."
The treatment room was a good choice, really. It was set up as a secondary OR to begin with, and while sticking a chest tube is a significant surgical procedure requiring anesthesia, sterile technique, and all the bells and whistles of surgery, it's still a fairly minor procedure.
"Evertson," he continued, "you ever stick a chest tube?"
"Only in the goat lab," I replied.
"Okay, you're it."
The Chief MAA began to splutter. He argued that as an "important witness," the injured sailor deserved the best of medical care, and shouldn't be used for "practice."
The Chief was, to be kind, a notorious bully and a pussy sickbay commando. A frequent flyer at sick call, he always demanded to see a "real" doctor. He was a fellow who wore his rank proudly, his badge heavily, and held his "inferiors" in obvious contempt. None of which had gone unnoticed.
LCDR Sharp gave the Chief a steely eyed glare.
"Uh, Sir," appended the Chief to his "I'm the one in charge here" statement.
"Out," said the surgeon.
The Chief left.
##########
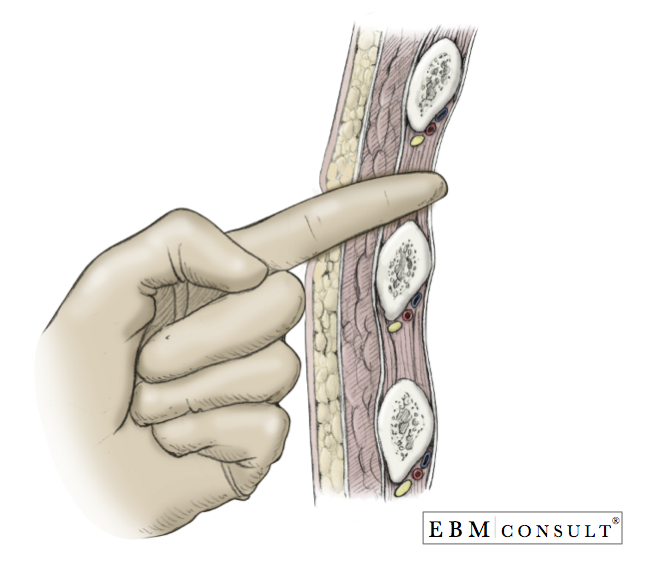
So, sticking a chest tube. It's not exactly putting on a bandaid, but it's really not that hard. You need to know your anatomy because there are a lot of potential pitfalls. There are nerves, veins and arteries running along the bottom of each rib, and getting into one or more of those could be catastrophic. Likewise, there's a diaphragm just a few centimeters below the place where you want to insert the tube, and a big honking liver lives down there too.
The whole idea of the chest tube is to put some negative pressure back into the pleural space. Or for the pedantically inclined, to remove the positive pressure. With the lung collapsed, there's space, air and positive pressure between the chest wall and the lung. If you stick a tube in there and connect it to suction all of the air (as well as any blood or other fluid) gets sucked out, pleural space pressure becomes negative, and the lung re-expands. Then it's just a matter of leaving the tube in long enough for the leaky places to heal over. The pleura and surrounding tissue is so highly vascular that healing happens, usually, in no more than a couple of days.
If you've done it right, you've dissected a path through the chest wall that will naturally (with a little bit of help) seal once the tube is withdrawn.
The procedure requires skill and knowledge but is generally straightforward and simple. It's pretty dramatic, too, both in the doing and in the result. It's challenging, satisfying and a lot of fun. That last is probably a head-scratcher to some folks, and I'm not sure I could explain it any better than this guy:
I'm not sure I ever thought about it as "being allowed to stab your patient," but again, I can't think of a way to describe the "funness" of sticking a chest tube.
##########
I wasn't at all surprised to be tasked with sticking the chest tube. In civilian land, where you can't swing a cat without hitting a surgeon, it's the kind of procedure that only surgeons do. But in the navy, on a warship, where there's a single surgeon and only 4-5 doctors total, you want your corpsmen to be trained to the highest level they can handle. I worked at a relatively high level and was constantly being trained in very advanced medical and surgical skills. So getting the nod was unsurprising and actually pretty much expected.
Here's how I did it.
The surgeon and I explained to the patient what was wrong, how we were going to fix it, and why. I asked him if he was comfortable with a corpsman doing the procedure.
"If it's you, no problem," he said, which was a nice pat on the back from a guy who had a lot of stuff on his plate and didn't need to be so kind.
He signed a consent form and we got to work. First I cleaned and scrubbed the surgical site, then carefully identified precisely where I would cut and marked it with a surgical marker. Then I applied betadine -- an iodine based bacteriostat -- to the skin. While the betadine was drying I scrubbed, gowned and gloved. The OR techs draped the patient, who was laying on his back with his right hand tucked behind his head. While this was going on LT Jones, the ship's nurse anesthetist, gave the patient a little bit of vitamin V (valium) through his IV.
Once the patient was relaxed I infiltrated the surgical site with two percent lidocaine with epinephrine, using a syringe and needle. Getting the anesthesia right is tricky and takes both time and a lot of attention to detail. You have to numb up not only the skin, but the underlying tissue as well. And there's a lot of it!

When I'd finished with the anesthesia and was satisfied with it, I called for tension on the skin at the incision site. The surgeon and one of the OR techs pulled the skin very taut, and I made a smooth, deep, three centimeter incision directly over the rib, opening the skin, subcutaneous tissue and muscle down to the periosteum. There was very little bleeding, thanks in part to the epinephrine in the anesthetic.
One of the MAA's, Reed or Malloy, went over like a bludgeoned ox. I was concentrating and didn't pay much attention, but someone dragged him out of the treatment room.

Next I called for a Kelly clamp,
and drove it through the intercostal musculature between the ribs. Opening the clamp, I pulled it back, bluntly dissecting the channel I was making until it was wide enough to slip my left index finger in. It was at about this point that the other MAA went down and was unceremoniously dragged away.

I did so and could feel the smoothness of the chest wall pleura. I left my finger in the hole and, using it as a guide, reinserted the Kelly until its tip was in contact with the pleura. Then I carefully drove the nose of the clamp through the pleura, which gave with a slight pop. It takes a lot of force to pop through the pleura!
My finger followed the Kelly through the pleura and I felt around, just to check for anything unusual. There might be a mass in there, for instance, or adhesions or scar tissue from pleurisy or a previous bout of pneumonia. There was nothing out of the ordinary. I didn't expect there to be, but you check anyway.
Next I called for the chest tube. I received a large Kelly clamp firmly clipped to the end of the tube.

Before the procedure we'd carefully measured the tube and marked it at the proper depth. We wanted the end of the tube to end up at the top, or apex, of the chest cavity, with the tube hugging the inside of the chest wall, so the mark was about 10-11 inches from the tip.
Again using my left index finger as a guide, I slid the Kelly and tube through the incision, between the ribs, and into the chest.

I released the Kelly, removed and discarded it, and carefully slid the tube in until the mark met the incision. As soon as I unclamped the tube air began to flow in and out of the tube with every breath the patient took. That's exactly the sign you want and tells you that your tube is indeed in the pleural space where it belongs. I removed my left finger and the OR tech hooked up the suction. After carefully observing the rise and fall of the water level in the suction device we concluded that the tube was correctly placed and that the lung and already re-expanded. Then I called for suture.

I placed a couple of mattress sutures which pulled the muscles, subcutaneous tissue and skin tightly closed around the tube. Then it was only a matter of applying an airtight dressing and we were done.

##########
A couple of days later the chest tube came out and the injured sailor was as good as new physically. He was probably not as good as new emotionally or legally. He left the ship on the COD only hours after being released from medical. Presumably he was heading for a court martial. I have no idea what ever became of him, and to be brutally honest, I never really thought about it. The entire episode pretty much vanished from my consciousness until I recently dug into a packet of old letters and was reminded.
##########
As you may recall, I was a little bit miffed at Danny's lack of performance during the emergency.
While I was waiting for the OR techs to get set up, I noticed that Danny had once again left his can of protein supplement powder (Choco-Powerlicious!) on the counter in the treatment room. Against clear orders to the contrary.
As you may also recall, Danny was a Real Weightlifter. I think he left his protein powder laying around to make sure that everyone knew and respected his status as a Real Weightlifter.
Next to the protein powder (Choco-Powerlicious!) was a box of hemoccult cards. Hmmm. I took out a card and flipped it open, exposing the two stool sample windows. I looked around a bit and found a bottle of betadine. I put on a rubber glove, dipped a finger in the betadine, and smeared it across the sample windows of the card. I considered the result for a moment, then shrugged. Looks like shit to me!
I closed up the card, tossed it in the protein powder, then shook the can up to cover the card. And promptly forgot about it.
A few weeks later an all hands muster was called in sickbay. Seems someone had placed a shit-covered hemoccult card in Dear Danny's protein supplement. The seniorish NCO running the muster allowed as how NIS had already identified the perp, and this would be the one and only opportunity for said perp to come forward, admit his crime, and perhaps be let off with only a Captains Mast. If the perp chose not to come forward, said the seniorish NCO, the hammer would fall. "This shit ain't funny," he said.
Well, you can guess what the perp didn't do. And like me, you might still be chuckling about the non-falling of the hammer.
##########
Now the aforementioned seniorish medical department NCO wasn't exactly the sharpest crayon on the box. You really had to wonder how he'd lived long enough and managed to not piss enough people off to make his exalted rank.
So one fine day, in the middle of morning sick call, a medical emergency was called away to hangar bay two. The medical response team responded, and soon the word came back that the victim was none other than the seniorish NCO fella. He'd cracked his head on a control surface and was bleeding spectacularly.
When he was delivered to medical he was trussed in a stokes stretcher with a cervical collar protecting his neck (just in case) and a bloody medium battle dressing atop his pate, tied securely tied beneath his chin. I pulled the battle dressing off to see how bad the scalp wound was. It wasn't, but it would need a few stitches. His next stop was x-ray to check for c-spine or skull fractures. I put a wad of sterile 4X4 sponges atop the wound and wrapped it in place with kerlex, then released him to x-ray.
The sponges I used in the dressing were cleverly equipped with radiopaque threads.

Such threads are designed to show up on x-ray so that sponges perhaps left inside the body after surgery might be found.
So the seniorish NCO's c-spine x-ray was fine, and so was his skull x-ray, although that one did clearly show the bright, squiggly lines of radiopaque thread superimposed on his hat holder.
As I was writing in the fellow's chart, he asked LCDR Smith what the squiggly lines on his x-ray were all about.
Under my breath, but not enough under my breath, I muttered, "That's the spirochete holding your two brain cells together."
I don't think the seniorish NCO heard me, but I know he wondered why two doctors, a nurse and a Warrant Officer erupted in uncontrollable laughter.
Chock full o' th' milk of human kindness, that's me.
Sick bay -- also known as H-Division or Medical -- was located right in the guts of the carrier. The hangar bay was the first, or "main" deck, and sick bay was below the hangar bay on the second deck, right on the centerline of the ship. Forward of sick bay was the forward galley and mess decks, and aft was -- perhaps unsurprisingly -- the aft galley and mess decks. Forward and aft of the mess decks there were scores of little shops and offices and vast berthing areas where hundreds of men lived in three-high "coffin" racks. A pair of fore-and-aft passageways ran the length of the second deck on each side -- port and starboard -- of sick bay.
As an aside, all of the "floors" from the hangar bay/main deck on down were called decks and numbered first, second, third, etc. Those above the main deck were called levels and were numbered oh-one, oh-two, oh-three, etc. The flight deck was the oh-four level.
 |
| No, I do not know why this Naval Reserve Intelligence diagram features F-16 lawn darts. S |
There aren't a lot of quiet moments on a warship on deployment. The quiet wouldn't last; as soon as the sun rose over the Holy Land we'd be leaving port. In a couple of hours they'd call away the special sea and anchor detail, raise the hook, and the carrier would depart Haifa and get on with all the navy stuff. For the moment, however, all was quiet. Most of the crew were snug in their racks, catching a few final hours of peaceful (in some cases ethanol induced) sleep before the onset of a busy underway period.
The two junior guys of the medical department watch section were playing cards in the medical records office.
 |
| Records office/counter. |
The section leader was in the pharmacy (he was the pharmacy tech) writing a letter.
 |
| Pharmacy. |
The rest of the watch section were crapped out on cots back aft in the medical ward.
 |
| Duty section back on the ward. That's a color tee-vee in the background! |
I finished stowing my gear and wandered into the treatment room to study.
 |
| Treatment room. |
I'd need to man the flight deck battle dressing station when they called away sea and anchor in a couple of hours, but for the moment I was comfortable in sick bay reading up on Mediterranean parasitology. Do you have any idea what mosquitoes put into you when they bite?
 |
| These. Plasmodium falciparum. |
I heard the portside sickbay door open and close, followed by low voices. Then a sudden shout. "Help!"
Oh shit.
##########
It was cruise number four for me, and fairly early in the deployment. We were back in the Mediterranean, and it was interesting times indeed.
U.S. aircraft carriers had been a constant presence in the Mediterranean since the end of WWII, protecting Europe's soft underbelly from Soviet aggression. That was our main brief, to be prepared to conduct war at sea against the Soviets, and, if it came down to it, to execute our part of the SIOP.
A lot of people have been katie couric'ed into believing that there was never really any cold war, just a bunch of hateful American imperialists swinging phallic symbols all over the place and oppressing the po' folk of the world. That the peaceful soviet peoples were simply building tractors and trying to bear up under the mean and racist policies of the evil George W. Hitler who was, at the time, working through his proxy-puppet Ronald Reagan. The Russians, so couric tells us, were far too poor to have a real military, and certainly didn't have a blue water navy.
 |
| Kresta II |
Those of us who were there know different. Though they had no aircraft carriers, the Soviets usually had as many, if not more, warships operating in the Med as the U.S. Navy. Cruisers and destroyers in the main...
 |
| Kynda |
 |
| Sovremennyy |
 |
| Udaloy |
 |
| Kashin |
 |
| AGI. Coral Sea in background. |
The AGI's were intelligence gathering platforms, often called "trawlers" by couric and her ilk, as if they were nothing more than peaceful commercial fishing vessels. We'll take a closer look at them in a future post.
The Soviets may have had no carriers (YAK-38/VTOL cruisers don't count, sorry), but that doesn't mean they lacked air power. There were significant naval aviation assets nearby in the Black Sea area, and the Soviets frequently operated aircraft out of Syria, Egypt, and Libya.
In reality, any U.S. - Soviet punching match in the Med would be a very big, very serious fight. And as if that wasn't enough...
There was Khaddafi in Libya. In addition to hosting a lot of Soviet airpower and allowing the Soviet navy port and maintenance facilities, he was exporting terror and constantly probing our Sixth Fleet defenses. That was the southern Med. In the east...
Lebanon. Just the name makes my palms sweat. There'd been a three-way civil war going on in Lebanon since 1958. Nothing is as it seems in that part of the world, though, so it was actually more like a 14- or 15-way civil war. Sunni and Shia, of course, Maronite Christians and Druze. Those were the locals. Then there were the illegal aliens; Palestinians and various exiled Islamic groups from Syria, Jordan and Iran. And let's not forget the commuters; military forces from Syria, Jordan, Egypt and Israel. There were contract mercenaries from Europe -- from both sides of the iron curtain -- and even mercenaries from America. And of course there were the big boys; the U.S. and France (Lebanon is a former French colony), each of which fielded both regular and special forces at various times. And the U.N. With the exception of the Iran-Iraq battlefields, Lebanon was the deadliest place on earth from about 1975-1995.
At the time this tale begins, various factions of an amorphous militant group called Islamic Jihad were keeping dozens of western hostages in and around Beirut. More than two dozen were American. There would also be a hijacking a few short weeks later, with the hostage-packed TWA 727 spending some time on the ramp at Beirut International. All of this Lebanese turmoil would mean that we'd spend most of our deployment in the eastern Med, and that I'd once again have the opportunity to visit the former "Pearl of the Mediterranean."
All of that was in the future and would come to overshadow the first weeks of the deployment, which had already been more eventful than usual.
##########
The morning we pulled into Haifa, I'd mustered with the rest of the Beach Guard detachment in hangar bay three. We'd be the first of the crew ashore and would set up a check point and control area at fleet landing. We'd be the ship's official presence ashore at the point where sailors on liberty would debark and embark from the liberty boats ferrying them ashore. The ship was far too large and drew too much water to come alongside the piers in the harbor.
Beach Guard was great duty. There were watches to stand, of course, and you had to be available for recall so no extended tours away from the city, but it also featured free lodgings in a nice hotel, generous per diem, and relief from regular one-in-three watch standing on the boat.
As we mustered on the hangar deck the ship's XO appeared and the Beach Guard OIC called us to attention.
"Okay fellas," said the XO, "when you get ashore there's going to be a lot of press with a lot of questions. Just tell 'em you don't know anything and refer 'em to the PAO. That should be easy, because you don't know anything, even if you've heard something or think you know something. Let me be very clear. You do not want me to read your name in the papers."
Well. This wan't my first rodeo, but the XO's little spiel was a first for me. I wondered what it was all about.
As promised, there was a lot of press ashore. The officers and Chiefs did a fine job of running interference for us, and I was a past master at looking like I was way to busy doing something really important to be bothered, so I was never in danger of being quoted.
Over the next few days we read the papers and listened to the scuttlebutt and gained some understanding of what had happened. Few, if any of us, had ever heard of or even seen Michael Walker.
Another thing we didn't know anything about was the fact that NIS (naval investigative service) had, on the first day of the port visit, cracked a drug ring on the ship. That was really a surprise to me, and actually made a bigger impression on me than the spy thing.
I was probably a real naif at the time (probably?!?) but when the CNO came out with "Not on MY watch, not on MY ship, not in MY Navy" I bought in completely. I knew there were dopers around, most of whom stuck out like a diseased tool. They were slovenly noloads as far as I could tell, and their behavior put me and my shipmates in mortal peril. I agreed wholly with the fleet solution to drug use. Send them firetruckers back to civilianland!
IIRC, Operation Golden-flow hit high gear back in '81, following the EA-6B crash on Nimitz. It slashed through the doper community like a scythe through rotting grain, and my fleet and my navy got better and better and better. By 1985 you just didn't see dopers anymore. Well, I didn't see dopers anymore. I'd pretty much forgotten all about them.
But they were still there...
##########
Now where was I? Oh yeah.
Oh shit!
I came left out of the treatment room and left again. This put me in the port-starboard transverse passageway that ran right through sickbay. The two duty corpsmen were huddled around a dungaree-clad sailor who was sitting on the deck with his back to the bulkhead.
 |
| The bulkhead behind the two sick call contestants at the counter. Note boom box. |
The two junior corpsmen were starting to panic. Neither worked in patient care; one was a medical supply clerk and the other worked in medical records.
The supply corpsman was standing back, looking at the blood on the wall with big eyes. I shall call him, for the purposes of this post, Danny Dumbf... er, Danny. He was a sawed-off, little banty rooster of a fellow who did a lot of weight lifting and had dreams of not getting sand kicked in his face ever again. The records corpsman was on his knees next to the slumped E-6, trying valiantly to blow a whistle.
Blow a whistle?
Yes, blow a whistle. At some point in the past, apparently, a lone corpsman had been presented with a middle-of-the-night emergency and had gone looking for help, leaving a sick or injured sailor to his own devices. Thereafter a shiny whistle was installed in the medical records office (first stop for anyone visiting sick bay) and everyone was instructed that should they find themselves in a similar situation, they should stay with the patient and blow the whistle to summon help.
But the poor records guy, who I shall call Bobby, couldn't work the whistle in his panic.
##########
Panic is one of those funny things. You simply can't be prepared for your first real emergency. You can know your stuff cold and have talked it through and thought it through and done drills out the wazoo, but the real thing is different.
My first real emergency was a simple one. I was still in Corps School (Basic Hospital Corps School) and doing a rotation on the wards at Balboa Naval Hospital. I was "assisting" Dr. Somthinerother who, if I was reading his shoulder boards correctly, was a freaking 0-5 Commander fer crying out loud! I was only a couple of weeks out of boot camp and the most senior officer I'd been this close to thus far in my career was an 0-3 Lieutenant. I'd only ever spoken to one officer, an Ensign, and the conversation had gone something like this:
"Are you getting enough chow, Recruit?"
"YESSIR!"
And here I was suddenly and unexpectedly rubbing shoulders with a Commander or Admiral or some shit!
Dr. Somthinerother had just given a patient a shot of demerol and the patient was trying very hard to stop breathing.
"Get me some narcan," snapped the Commander.
I panicked. I knew instantly that this was an emergency. But I had no idea what narcan was; whether it was medicine or medical gear or sandwich spread. I'd clearly been given an order, and it was clearly a damned important order, but I didn't know what it meant and I didn't know what to do. I stood there, rooted to the ground, mind spinning uselessly, and doing absolutely firetruck-all.
The Commander looked at me, rolled his eyes, and bellowed.
"NURSE, NARCAN!"
Well, Nurse JayGee knew what narcan was and came dashing in to save the day. For the patient, anyway. As for me, I had visions of suddenly becoming a non-designated Seaman Recruit and spending the next four years chipping paint.
Later Nurse JayGee gave me a stern but kindly lecture about emergencies and panic. Which I took to heart.
##########
"Arright," I said, "let's get him in the treatment room." I bent down and grabbed the injured fellow's arm.
I'd already done a quick and dirty field assessment. He was conscious and alert, probably more scared than in genuine pain. He was breathing spontaneously and well, and while he was obviously bleeding, he wasn't bleeding a lot, at least externally. We really needed to get him into the treatment room and onto an exam table, the sooner the better. There was no need to go through all the stretcher rigmarole to move him 30 feet, and the way he moved would provide more detail for my initial assessment.
Bobby and I got the fellow up and moved into the treatment room. I sent Danny to call the duty doc, CDR Portly. I helped the injured guy out of his shirt and had Bobby start taking vital signs. Then I got my first look at the wound.
It was a half-inch slit, about 5-6 inches down from the top of the back, 3 inches to the right of the spine, just slightly above and to the left of the lower point of the shoulder blade. The wound had already stopped bleeding. With every breath the fellow took, though, a couple of bloody bubbles formed in the wound.
Ruh-roh. Sucking chest. Not a bad one -- at least not yet -- but a sucking chest wound nonetheless. Now how in the hell...
"What happened?"
"Motherfucker stab me."
A quick game of 20 questions revealed that the guy had been getting up for watch from his rack in one of the 99-man berthing areas. For some reason all the lights were out, and as he stumbled around someone had knifed him in the back, then fled.
Well shit! A firetrucking stabbing? Here, on the boat? WTF?
"Danny, call the MAA's. And where the hell is CDR Portly? What did he say when you called him?"
As it turned out, Danny hadn't called the duty doc at all. The whining excuses began to flow.
"Never mind," I said, "Go get HM1 Pharma, ask him to come to the treatment room. Do you understand that? Where are you going to bring HM1 Pharma?"
"Yes. Treatment room." Pouting and sullen.
I picked up the phone. I called CDR Portly first.
"Sorry to bother you, Doc, but we got a guy down here who's been stabbed in the back."
"Whaa..., what?"
"Got a guy with a sucking chest, he's been stabbed in the back."
"In the back of what?"
"In the back of his front! Oh, hell, never mind."
I hung up and called LCDR Sharp, the Ship's Surgeon. He was the one we really needed anyway, and Portly would likely just slow things down and firetruck things up.
"Be right there," said the surgeon.
The section leader rolled in with Danny in trail. I briefed him, then picked up the phone to call the MAA's.
"In the back of what?"
Firetruck me, I thought, this is gonna be one of those days.
##########
Sucking chest wound. Here's how it works.
Your lungs are, obviously, in your chest cavity. The left one has two lobes, the right one has three. For our purposes we'll just consider them to be two lungs. They're connected to the outside via the windpipe, which leads to the mouth and nose. Inside the lungs the windpipe branches and branches and branches, becoming the bronchus, the bronchial tubes, and finally the alevoli, teeny-tiny sacs where oxygen and carbon dioxide are exchanged. Far from being hollow balloons, the lungs are actually fairly solid organs, filled with passageways, blood vessels, and specialized tissues. They're obviously less solid than other organs, and just as obviously hold a lot of air (even when you try to blow it all out), but they're much more than simple air-filled bags.
Now whether you're breathing in or out, whether you've taken a deep breath or have exhaled every bit of air you can, your lungs remain fully expanded in the chest cavity, filling it completely. The thing that allows you to breathe in and out, to take air into the lungs and exhale air out of the lungs, is a simple change in the geometry of the inside of the chest. When you breathe in, the diaphragm pulls down, expanding the volume of the chest cavity. When the volume expands, the pressure inside the chest falls, and air flows in. When you exhale, the reverse happens.
As noted before, the lungs are always completely expanded in the chest cavity, taking up the entire space allotted to them. This is because there is always a slightly negative pressure in the pleural space, which lies between the outside of the lung and the inside of the chest wall. The pleura is the specialized tissue which lines the inside of the chest cavity and the outside of the lungs. It's quite tough and air tight and continually secretes a lubricating fluid which allows the lung and chest wall to move against each other with very little friction. The slight negative pressure in the pleural space between the lung and the chest wall keeps the lungs ever expanded.
So the lungs are always expanded, except when that negative pressure in the pleural space is lost. That can happen in two ways. The lung can leak air into the pleural space, or some kind of trauma (a knife wound, for instance) can allow air from the outside to leak into the pleural space. In some instances (like a knife wound), the trauma might do both, letting in outside air as well as inside air from a damaged lung.
 |
| Pneumothorax and fix. Stolen from the interwebs. |
When air leaks into the pleural space and the negative pressure is lost the lung can no longer remain completely expanded in the chest and it begins to collapse. As long as air can move freely in and out of the pleural space, the lung can still function, after a fashion, but at greatly reduced efficiency. However, if air builds up in the pleural space the increased pressure will eventually crush the lung to uselessness, and if it continues unchecked can actually squeeze the heart, great vessels of the chest, and the other lung into uselessness too. Which is bad.
Trauma can also allow blood to fill the pleural space, and since liquids don't compress, this condition can be much more severe and can happen very rapidly.
If there's air in the pleural space, the condition is called a pneumothorax. If it's blood, it's called a hemothorax. If both air and blood, it's a pneumo-hemothorax. If pressure builds up it's a tension pneumo, hemo, or pneumo-hemothorax. In any combination the lay term is collapsed lung, and in any combination it's a very serious condition and generally treated as a medical emergency.
##########
On exam the guy was an otherwise healthy male, about 30 years old. His vital signs were normal with the exception of a slightly fast pulse, about 100 beats per minute. He was alert and oriented and answering questions. He acted a little more depressed than excited. He kept his face mostly pointed toward the deck and didn't want to make eye contact.
Other then the wound in his back he had no injuries. When I listened to his chest I could hear good breath sounds on the left but no breath sounds on the right. His heart sounded good. His trachea was midline, which was good. If pressure was building in his chest the trachea would eventually begin to shift shift. It looked very much like he had a relatively uncomplicated traumatic pneumothorax. He'd been very lucky.
The pneumothorax was still going to have to be fixed, though, So I went ahead and started an IV and drew labs. I sent Bobby off to wake up the lab tech and the x-ray tech.
LCDR Sharp rolled in, examined the injured sailor, and reached the same conclusions I had. Which is not to say that my conclusions were in anyway brilliant. It was pretty darned obvious.
Dr. Sharp wanted to take the guy to OR to fix the problem, so he sent Danny off to round up some OR techs and picked up the phone to call LT Jones, the ship's nurse anesthetist.
"Do we have x-rays yet?"
About that time Bobby rolled back in with the lab tech and reported that the x-ray tech was still too drunk to function.
Which wasn't any real problem, because I could shoot and develop the chest films. Which I did (If you'd like to see a slideshow of chest radiography, this is a pretty good one). When I brought the x-rays out of the darkroom, however, the treatment room was crowded with MAA's and a number of rather senior officers. It was pandemoneous!
Listening to the conversations and to the questions the MAA's were asking the injured sailor, it didn't take long to figure out what was going on. Our patient was one of the guys snapped up in the drug investigation and had been "cooperating with the authorities." Apparently this was not appreciated by some segment of the ship's drug culture. Which had heretofore been completely invisible to me.
To the me of that place and that time, the whole thing was shocking and confusing. I suppose that at some intellectual level I realized that in any small town of 6,000 souls there would be some lawbreakers. But for god's sake, murderers? There were people on my boat who would actually kill a shipmate, or at least give it the old college try? Good lord! The situation was an eye opener and, in some ways, one of the more painful lessons of growing up.
It was rather amusing to watch and listen to the ship's crack team of investigators though. MAA's, or Master at Arms, are the navy's police force. I think things have changed a lot since 1985, and I can't speak to today's practices, but back then most of the ship's MAA force were temporarily assigned to the duty and received a very basic level of training, followed by OJT. Only very senior MAA's received formal training, and my guess is that such training was weighted more toward the administrative aspects of law enforcement rather than the investigative.
The upshot, IMO, was that in a "big" and "exciting" situation such as attempted murder, our MAA force turned into a bunch of kids playing cops and robbers. That's not to say they weren't competent or that they weren't doing a fine and necessary job, but I'm here to tell ya that the treatment room was awash with all the cop characters from ADAM-12 and Dragnet that morning.
##########
We still had an injured sailor to deal with, so the surgeon invited all the giddy pseudo cop thespians to take their show on the road. The Chief MAA couldn't keep himself from playing a couple of rounds of "who's the big dog," which he lost. As a concession, he was allowed to leave two of his men behind to provide "security" and to record the patient's "dying declaration." If it came to that. Which it wouldn't, but the Chief was a big fan of ADAM-12.
"Well," said Dr. Sharp, "If officers Malloy and Reed are gonna be here, we can't use the OR. Not enough room. So we'll do it here in the treatment room."
The treatment room was a good choice, really. It was set up as a secondary OR to begin with, and while sticking a chest tube is a significant surgical procedure requiring anesthesia, sterile technique, and all the bells and whistles of surgery, it's still a fairly minor procedure.
"Evertson," he continued, "you ever stick a chest tube?"
"Only in the goat lab," I replied.
"Okay, you're it."
The Chief MAA began to splutter. He argued that as an "important witness," the injured sailor deserved the best of medical care, and shouldn't be used for "practice."
The Chief was, to be kind, a notorious bully and a pussy sickbay commando. A frequent flyer at sick call, he always demanded to see a "real" doctor. He was a fellow who wore his rank proudly, his badge heavily, and held his "inferiors" in obvious contempt. None of which had gone unnoticed.
LCDR Sharp gave the Chief a steely eyed glare.
"Uh, Sir," appended the Chief to his "I'm the one in charge here" statement.
"Out," said the surgeon.
The Chief left.
##########
So, sticking a chest tube. It's not exactly putting on a bandaid, but it's really not that hard. You need to know your anatomy because there are a lot of potential pitfalls. There are nerves, veins and arteries running along the bottom of each rib, and getting into one or more of those could be catastrophic. Likewise, there's a diaphragm just a few centimeters below the place where you want to insert the tube, and a big honking liver lives down there too.
The whole idea of the chest tube is to put some negative pressure back into the pleural space. Or for the pedantically inclined, to remove the positive pressure. With the lung collapsed, there's space, air and positive pressure between the chest wall and the lung. If you stick a tube in there and connect it to suction all of the air (as well as any blood or other fluid) gets sucked out, pleural space pressure becomes negative, and the lung re-expands. Then it's just a matter of leaving the tube in long enough for the leaky places to heal over. The pleura and surrounding tissue is so highly vascular that healing happens, usually, in no more than a couple of days.
If you've done it right, you've dissected a path through the chest wall that will naturally (with a little bit of help) seal once the tube is withdrawn.
The procedure requires skill and knowledge but is generally straightforward and simple. It's pretty dramatic, too, both in the doing and in the result. It's challenging, satisfying and a lot of fun. That last is probably a head-scratcher to some folks, and I'm not sure I could explain it any better than this guy:
I'm not sure I ever thought about it as "being allowed to stab your patient," but again, I can't think of a way to describe the "funness" of sticking a chest tube.
##########
I wasn't at all surprised to be tasked with sticking the chest tube. In civilian land, where you can't swing a cat without hitting a surgeon, it's the kind of procedure that only surgeons do. But in the navy, on a warship, where there's a single surgeon and only 4-5 doctors total, you want your corpsmen to be trained to the highest level they can handle. I worked at a relatively high level and was constantly being trained in very advanced medical and surgical skills. So getting the nod was unsurprising and actually pretty much expected.
Here's how I did it.
The surgeon and I explained to the patient what was wrong, how we were going to fix it, and why. I asked him if he was comfortable with a corpsman doing the procedure.
"If it's you, no problem," he said, which was a nice pat on the back from a guy who had a lot of stuff on his plate and didn't need to be so kind.
He signed a consent form and we got to work. First I cleaned and scrubbed the surgical site, then carefully identified precisely where I would cut and marked it with a surgical marker. Then I applied betadine -- an iodine based bacteriostat -- to the skin. While the betadine was drying I scrubbed, gowned and gloved. The OR techs draped the patient, who was laying on his back with his right hand tucked behind his head. While this was going on LT Jones, the ship's nurse anesthetist, gave the patient a little bit of vitamin V (valium) through his IV.
Once the patient was relaxed I infiltrated the surgical site with two percent lidocaine with epinephrine, using a syringe and needle. Getting the anesthesia right is tricky and takes both time and a lot of attention to detail. You have to numb up not only the skin, but the underlying tissue as well. And there's a lot of it!

When I'd finished with the anesthesia and was satisfied with it, I called for tension on the skin at the incision site. The surgeon and one of the OR techs pulled the skin very taut, and I made a smooth, deep, three centimeter incision directly over the rib, opening the skin, subcutaneous tissue and muscle down to the periosteum. There was very little bleeding, thanks in part to the epinephrine in the anesthetic.
One of the MAA's, Reed or Malloy, went over like a bludgeoned ox. I was concentrating and didn't pay much attention, but someone dragged him out of the treatment room.

Next I called for a Kelly clamp,
 |
| Kelly |
and drove it through the intercostal musculature between the ribs. Opening the clamp, I pulled it back, bluntly dissecting the channel I was making until it was wide enough to slip my left index finger in. It was at about this point that the other MAA went down and was unceremoniously dragged away.
I did so and could feel the smoothness of the chest wall pleura. I left my finger in the hole and, using it as a guide, reinserted the Kelly until its tip was in contact with the pleura. Then I carefully drove the nose of the clamp through the pleura, which gave with a slight pop. It takes a lot of force to pop through the pleura!
My finger followed the Kelly through the pleura and I felt around, just to check for anything unusual. There might be a mass in there, for instance, or adhesions or scar tissue from pleurisy or a previous bout of pneumonia. There was nothing out of the ordinary. I didn't expect there to be, but you check anyway.
Next I called for the chest tube. I received a large Kelly clamp firmly clipped to the end of the tube.

Before the procedure we'd carefully measured the tube and marked it at the proper depth. We wanted the end of the tube to end up at the top, or apex, of the chest cavity, with the tube hugging the inside of the chest wall, so the mark was about 10-11 inches from the tip.
Again using my left index finger as a guide, I slid the Kelly and tube through the incision, between the ribs, and into the chest.

I released the Kelly, removed and discarded it, and carefully slid the tube in until the mark met the incision. As soon as I unclamped the tube air began to flow in and out of the tube with every breath the patient took. That's exactly the sign you want and tells you that your tube is indeed in the pleural space where it belongs. I removed my left finger and the OR tech hooked up the suction. After carefully observing the rise and fall of the water level in the suction device we concluded that the tube was correctly placed and that the lung and already re-expanded. Then I called for suture.

I placed a couple of mattress sutures which pulled the muscles, subcutaneous tissue and skin tightly closed around the tube. Then it was only a matter of applying an airtight dressing and we were done.

##########
A couple of days later the chest tube came out and the injured sailor was as good as new physically. He was probably not as good as new emotionally or legally. He left the ship on the COD only hours after being released from medical. Presumably he was heading for a court martial. I have no idea what ever became of him, and to be brutally honest, I never really thought about it. The entire episode pretty much vanished from my consciousness until I recently dug into a packet of old letters and was reminded.
##########
As you may recall, I was a little bit miffed at Danny's lack of performance during the emergency.
While I was waiting for the OR techs to get set up, I noticed that Danny had once again left his can of protein supplement powder (Choco-Powerlicious!) on the counter in the treatment room. Against clear orders to the contrary.
As you may also recall, Danny was a Real Weightlifter. I think he left his protein powder laying around to make sure that everyone knew and respected his status as a Real Weightlifter.
Next to the protein powder (Choco-Powerlicious!) was a box of hemoccult cards. Hmmm. I took out a card and flipped it open, exposing the two stool sample windows. I looked around a bit and found a bottle of betadine. I put on a rubber glove, dipped a finger in the betadine, and smeared it across the sample windows of the card. I considered the result for a moment, then shrugged. Looks like shit to me!
I closed up the card, tossed it in the protein powder, then shook the can up to cover the card. And promptly forgot about it.
A few weeks later an all hands muster was called in sickbay. Seems someone had placed a shit-covered hemoccult card in Dear Danny's protein supplement. The seniorish NCO running the muster allowed as how NIS had already identified the perp, and this would be the one and only opportunity for said perp to come forward, admit his crime, and perhaps be let off with only a Captains Mast. If the perp chose not to come forward, said the seniorish NCO, the hammer would fall. "This shit ain't funny," he said.
Well, you can guess what the perp didn't do. And like me, you might still be chuckling about the non-falling of the hammer.
##########
Now the aforementioned seniorish medical department NCO wasn't exactly the sharpest crayon on the box. You really had to wonder how he'd lived long enough and managed to not piss enough people off to make his exalted rank.
So one fine day, in the middle of morning sick call, a medical emergency was called away to hangar bay two. The medical response team responded, and soon the word came back that the victim was none other than the seniorish NCO fella. He'd cracked his head on a control surface and was bleeding spectacularly.
When he was delivered to medical he was trussed in a stokes stretcher with a cervical collar protecting his neck (just in case) and a bloody medium battle dressing atop his pate, tied securely tied beneath his chin. I pulled the battle dressing off to see how bad the scalp wound was. It wasn't, but it would need a few stitches. His next stop was x-ray to check for c-spine or skull fractures. I put a wad of sterile 4X4 sponges atop the wound and wrapped it in place with kerlex, then released him to x-ray.
The sponges I used in the dressing were cleverly equipped with radiopaque threads.

Such threads are designed to show up on x-ray so that sponges perhaps left inside the body after surgery might be found.
So the seniorish NCO's c-spine x-ray was fine, and so was his skull x-ray, although that one did clearly show the bright, squiggly lines of radiopaque thread superimposed on his hat holder.
 |
| Not a hat holder. The sponge is actually in a uterus here. Strangely appropriate. |
As I was writing in the fellow's chart, he asked LCDR Smith what the squiggly lines on his x-ray were all about.
Under my breath, but not enough under my breath, I muttered, "That's the spirochete holding your two brain cells together."
 |
| Spirochetes. |
I don't think the seniorish NCO heard me, but I know he wondered why two doctors, a nurse and a Warrant Officer erupted in uncontrollable laughter.
Chock full o' th' milk of human kindness, that's me.
##########
Be well and embrace the blessings of liberty.
And THAT was priceless!
ReplyDeleteI experienced the drug sweeps both on Okinawa, in Korea, and at my first Stateside assignment in Denver. In Denver Operation Golden Flow swooped through our maintenance squadron and bagged three victims from my shop. Unbelievable what the kids thought they could get away with. One of 'em was actually "mine," a very smart and talented lady who could have gone far. Off duty she thought the world was Grand Theft Auto before there was such a thing. Surprised the Hell out of me.
Some of my airmen caught Hell for not tipping me off sooner. Perhaps she could have been saved before she went down that road. All for naught though, all three airmen were unceremoniously discharged.
Interesting times, though the drug scene at Kadena was far worse, it was right after Vietnam and let's just say, things were strange indeed.
Great story Shaun, and now I know how brain cells, two each, are connected.
Yep, like much of human anatomy and physiology, it's all pretty simple! :)
DeleteI'm a complete libertarian when it comes to drugs. As far as I'm concerned, you wanna do 'em, it's a free country and you should be able to do 'em. Choices come with consequences, however, and you really can't mix drug use with certain jobs. It's fine for bureaucrats and kongrasskritters and mailmen and mary kay salesmen, and so on and so forth. But not for military, cops, astronauts, or other jobs requiring a clear mind and 100+ percent dedication. So I didn't have any problem with the military drug purges. You wanna stay in, stay clean. Do drugs, get caught, go home. Your choice.
The down side of course is that people "ruined" their service and perhaps their lives by making bad decisions and acting on them. That's too bad and I recognize it. But the other side of the coin is the impact their selfish behavior had on their shipmates and fellow servicemen.
Life is a trial. It's amusing to me that in this day in age nearly all 'merkins have declared themselves to be professional victims and spend much of their time pointing fingers of blame at everyone who comes close. They always fail too see the three fingers they're pointing at themselves, and fail to recognize that we shoot ourselves in the foot far more frequently than we're ever victimized by others.
Whoops, that was a rant!
Wonderful story. I love reading these. I learn something new every time.
ReplyDeleteThanks Marc. I'll try to keep 'em coming.
Delete